
|
Getting your Trinity Audio player ready...
|
By Halima Gongo
Kwale County, Kenya: In villages across Kwale County, Kenya, a Pap smear is nicknamed “kukorogwa”, in the Swahili language, “to be stirred.”
The word, which carries embarrassment and fear, comes from the sound of a speculum being locked during the examination that screens for cervical cancer.
“When you are locking the speculum, it makes a sound like drilling. Most women say they are afraid of being tortured with the drill. That is where the term ‘kukorogwa’ comes from,” explains Evelyne Nyanduko, a nurse at Kinondo Kwetu Hospital.
Conversations about reproductive health are taboo, and the screening process—requiring physical exposure—can feel deeply uncomfortable in conservative rural communities. The result is silence and avoidance that keeps many women away from hospital screening rooms until their bodies force them to go.
Fatuma Salim, 58, has never had a Pap smear done. The mother of four has only heard about the disease in whispers, but she fears the unfamiliar process of screening as much as the disease.
“I have just heard people talk about it. Some of my relatives have died because of cervical cancer. But I don’t know how the testing is done. I just know it has no cure,” Fatuma says calmly.
But fear is only part of the story, as structural barriers also stand in the way. Health facilities are often far from rural homes, and costs are high, making screening a lower priority compared to immediate illness. Many women also lack access to information and support to seek care. In some households, women must negotiate permission or money from their partners before going to a health facility. As a result, screening is delayed until symptoms become severe, and many women are diagnosed at advanced stages of cancer, when treatment options are limited.
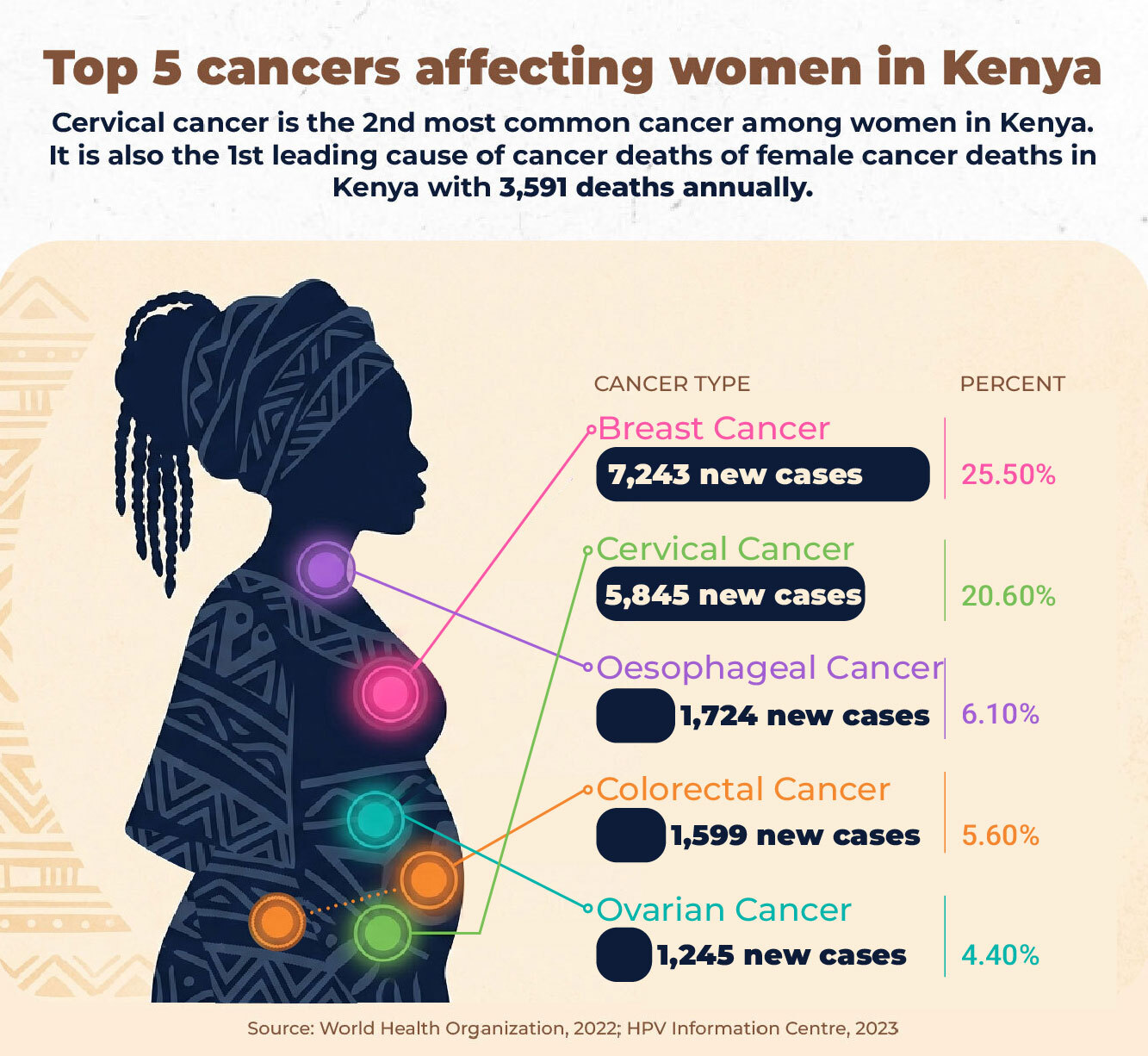
According to Kenya’s Ministry of Health, the country records about 5,845 new cervical cancer cases each year, with 3,591 deaths annually. It is the second most common cancer among women in Kenya and the leading cause of cancer deaths among women.
Despite this, only about 16.8 per cent of women in Kenya have ever been screened, reflecting gaps in access to preventive healthcare.
Globally, the World Health Organization estimates that 660,000 women were diagnosed with cervical cancer in 2022, and 350,000 died, with nearly 90 per cent of cases occurring in low- and middle-income countries.
In Kwale County, where more than 860,000 people are spread across vast rural areas, access to screening remains limited.
For years, many women in Kwale have largely depended on Kinondo Kwetu Hospital for cervical cancer screening. The hospital receives referrals from dispensaries, private clinics, and sub-county hospitals. But even when women made it there, the process was slow.
According to Harrison Kaingu, Chief Executive Officer of Kinondo Kwetu Hospital, coastal Kenya has only about six pathologists serving more than six million people, while Kwale County has just one. As a result, thousands of women rely on a very limited number of specialists to review their results, often leading to delays.
“In Kwale County in general, the HPV cases have not yet been quantified because of the lack of testing devices. We still do not have the HPV DNA testing site in Kwale. We rely on Mombasa,” he explains.
HPV, the human papillomavirus, is the main cause of cervical cancer. Without widespread testing, the true burden remains unclear.
While traditional methods such as Visual Inspection with Acetic Acid (VIA) and Visual Inspection with Lugol’s Iodine (VILI) have played an important role, they come with limitations.
“There are a few drawbacks to VIA/VILI, one being the expertise and accuracy of the test,” he says.
Under the old system, Visual Inspection with Acetic Acid (VIA) and Visual Inspection with Lugol’s Iodine (VILI) depended heavily on the examiner’s skill, and Pap smear slides were manually examined under a microscope by a specialist.
Slides and samples would pile up; patients would wait, sometimes one to two months, sometimes longer, before receiving results. Women who travelled long distances, paid for transport, and overcame cultural fears just to be screened faced crushing delays.
Kaingu says many women, tired of waiting, turned to alternative remedies or simply chose not to follow up at all.
To address these challenges, Kinondo Kwetu Hospital introduced AI-assisted digital microscopy (Euphoria) for Pap smear analysis. The technology reduces the wait time between testing and diagnosis, enabling faster detection of cancerous cells.
The system screens slides and highlights potentially abnormal cells, allowing pathologists to prioritise cases more efficiently.
The AI-assisted digital microscopy (Euphoria) in Kinondo Kwetu Hospital began as a pilot study in 2019. The system was trained on over 30,000 images and initially used as a research tool, but it is now being developed for point-of-care use.
Euphoria screens slides, highlighting likely abnormal cells, and significantly reduces the workload of the few available pathologists. Only the slides flagged as suspicious are prioritised for human review, ensuring efficiency without compromising accuracy.
The system is cloud-based with secure storage, allowing results to be verified remotely by qualified pathologists.
“We have one pathologist for over 700,000 people. If you consider the eligible population, that goes to almost 200,000 women who need to be screened. Among that population are HIV-exposed women, who are at higher risk. Using AI-assisted digital microscopy, we have trained the system called ‘Euphoria’ for Artificial Intelligence for image analysis to make an accurate diagnosis of cervical cancer. It has now shown accuracy of up to 99 per cent.”
However, these accuracy claims are largely based on internal data, and independent large-scale verification is limited.
Caroline Ngute, a registered oncology nurse in Kwale County, says the technology shows promise but must be used with caution. She explains that many AI systems are trained on data that does not fully represent African women. This introduces the risk that some conditions may be missed or misinterpreted, potentially reinforcing existing health inequalities.

“AI can improve diagnosis, especially where we have very few pathologists. But it also comes with risks and limitations; there is a risk of false results or biased interpretation. What the system learns may not fully match what we see on the ground,” she adds.
She also raises concerns about patient data and consent.
“We must ensure patient privacy and informed consent; without strong protections, these systems can expose sensitive health data. These are real people, and their data must be protected. Also, healthcare workers need proper training, and there is a risk of overreliance on the system if we are not careful,” she explains.
The technology behind Euphoria comes from Helsinki, Finland. Kinondo Kwetu collaborates with the Karolinska Institute in Sweden, the Finnish Institute of Molecular Medicine, and the Technical University of Mombasa to develop and refine the AI system for cervical cancer screening in Kenya. While these partnerships bring technical expertise, they also highlight an imbalance in who designs, owns, and governs AI systems used in healthcare in Kenya. It’s not clear how much control local institutions have over the technology, where the data is stored, how it flows across borders, and whether Kenya is building long-term local capacity.
There are also questions about how informed consent is obtained, whether patients fully understand that AI systems may analyse their samples, and who ultimately has access to this data beyond the hospital.
“Patient data is secure, fully compliant with the Data Protection Act, and stored in the cloud. Access to Euphoria is limited to authorised personnel with verified expertise. We don’t use patient names; only coded identifiers, and we can retrieve results whenever the patient needs them, even years later.” Kaingu says.
For women like Rosemary Kamau, a resident of Ukunda, the difference is tangible. Her results came in a day after the samples were taken. She also didn’t have to go back to the hospital for the results; the hospital called her.
“They called me at home and told me my results were in, even though I hadn’t gone to pick them up. The follow-up was fast, and it didn’t feel like waiting for months,” she says.
The cost of screening has also reduced significantly, making it more accessible. Under the conventional Pap smear system, a single test could cost about Sh5,000, a steep price for many families in rural Kwale. With AI-assisted digital microscopy, the cost has been cut by more than half to about Sh2,000.
“The other cost is for items like brushes, stains, and slides. That can also be reduced by half with this tool,” says Kaingu.
So far, Kinondo Kwetu Hospital has screened over 1,500 women using the AI-assisted system; 38 were treated for precancerous lesions, while five were found to already have cervical cancer.
For years, women like Fatuma feared what they could not understand. Today, diagnosis is faster and within reach. But even with this progress, many women are still navigating issues of access, trust, and dignity in their care.
While AI is improving efficiency, making cervical cancer screening faster, it does not fully address the barriers that prevent many women from accessing care in the first place. For many women, cost, distance, stigma, limited autonomy over their health decisions, and access to treatment remain unchanged. As the technology expands, it needs to do so equitably, transparently, and with informed consent.
This article was produced as part of the Gender+AI Reporting Fellowship, with support from the Africa Women’s Journalism Project (AWJP) in partnership with DW Akademie. The journalist used AI tools as research aids to review and summarise relevant policy and research documents and extract key statistics. All interviews, analysis, editorial decisions, and final wording were done by the reporter, in line with Talk Africa’s editorial standards.













{kind=link}